By Michael Butler, Jeffery Ni, and Anastasia Nicolov 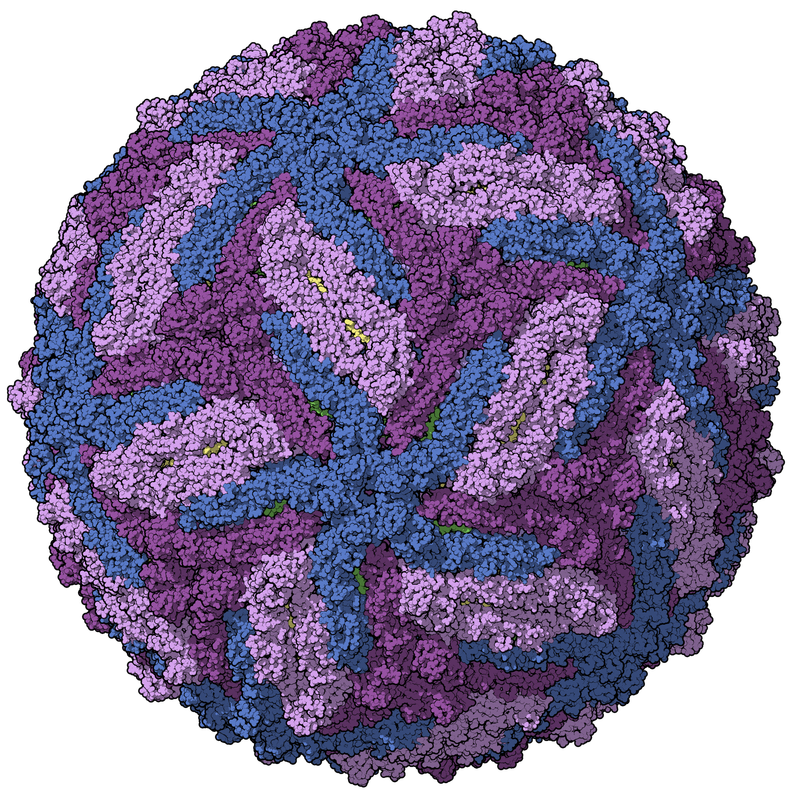 Each year, news reports herald the latest infectious disease scare. In the last few months, Zika virus has been on the forefront of the public’s awareness, with concerns over the safety of Rio’s Summer Olympics and calls from South American governments to postpone pregnancy until further notice in order to curtail side effects of the disease [1]. Within recent memory, Ebola virus, swine flu, and SARS have all posed global threats. Without first-hand experience and expert understanding of these diseases, it is difficult to sort out truth from hype. However, one thing is certain: vaccines have and continue to protect vast numbers of people from the devastating effects of infectious diseases. One of the greatest marvels of modern medicine, vaccines have in the last century led to the complete eradication of diseases like smallpox, as well as the near-elimination of polio, hepatitis A and B, and measles in the Western world [2]. Inoculation against chicken pox, whooping cough, and the seasonal flu save thousands of lives each year in the United States, and widespread vaccination has led to herd immunity, dramatically reducing disease risk for the most vulnerable members of the population – those who are medically unable to be vaccinated or who are immunosuppressed. Despite the clear benefits of vaccines, few people have more than a superficial understanding of how they work or the enormous effort that goes into making them safe and effective. Here, we hope to give insight into the vaccine production process as well as recent innovations. Basic Immunology As the body’s most intricate line of defense, the immune system is comprised of cells that recognize the difference between self and foreign entities in our body and target foreign or abnormal particles for elimination from the body [3]. While there are numerous cell types, lymphocytes (namely, B and T cells) are the most involved with targeted responses to specific diseases. Commonly referred to as white blood cells, these cells find and destroy disease particles, known as pathogens. Some of these cells contain a memory component; they are long-lasting in the body and produce antibodies that are able to recognize that particular pathogen again. This speeds up the process of elimination in future exposures, preventing extensive damage caused by the disease. Essentially, vaccines stimulate this memory response without the presence of the disease-causing element [3]. Vaccines in widespread use generally come in two different types: live attenuated virus vaccines and inactivated virus vaccines. Live attenuated viruses are viruses that are modified so as not to present danger to humans. Inactivated viruses are viruses that have been killed through heat or a chemical reaction. In summary, when a vaccine is injected into the body, it produces an immune response, but no illness occurs because the malignant components of the virus are not functioning. Epidemiology and Virus Identification Whenever a new illness is observed in the public, particularly one that spreads easily to others and causes severe symptoms, a highly-trained group of disease experts and biological scientists descends on the affected region with the goal of creating a vaccine. The United States Centers for Disease Control (CDC) and the World Health Organization (WHO) are two organizations that play key roles in this process. The term “epidemic” carries a weight in the public vernacular indicative of a great, impending danger. Although this may be true in some cases, the term is quite loosely defined. The CDC is responsible for determining what constitutes an epidemic in the United States [4]. It collects data on trends in disease statistics and constantly has a team of analysts gauging fluctuations from the norm. When statistics such as morbidity or incidence of a certain disease are above what is expected for an extended period, the CDC officially deems the event an epidemic. The WHO has a similar role in disease identification on a global scale [5]. For viruses with constantly mutating strains like influenza, the WHO has built a network of laboratories that routinely collect blood samples from patients infected with the circulating strain in order to start development of a new vaccine. For new epidemics, collection of blood samples occurs upon identification of a threat. From these samples, viruses are isolated and purified in order to create a laboratory stock. From this, a new vaccine can be developed. Vaccine Development From the isolated strain, a modified “vaccine virus” must be created [5]. Methods for doing this vary depending on the disease, but in most cases, the virus is made less dangerous by identifying and mutating regions that cause severe reactions in humans. Modifications may also be made to improve growth efficiency in certain conditions to ease translation to large-scale manufacturing. For example, with the flu vaccine, the vaccine virus is better able to grow in chicken eggs, as this is the standard manufacturing protocol. Next, the vaccine must be extensively tested in vitro (using living cells in a dish) and in vivo (in living animals) to ensure that it produces an immune response without a dangerous reaction [5]. This is easier said than done, as each disease has a different set of challenges. For example, rabies vaccines use inactivated viruses, so ensuring the viruses stay inactive is a top priority. Pneumococcal pneumonia has multiple strains, all of which need a different chemical conjugation method before they are blended into one vaccine. Hepatitis B vaccine viruses are difficult to produce efficiently and consistently in the lab. Depending on the virus and vaccine type, growth conditions may need to be optimized and vaccines modified with additives [5]. For example, many vaccines include adjuvants, which are chemicals that help stimulate a larger immune response. If the WHO is involved, a set of standards is developed that helps vaccine manufacturers measure how much vaccine they produce and ensure that dosing remains correct and consistent throughout their stock. Vaccine Manufacturing While hundreds of companies worldwide produce vaccines for many diseases, this production is usually on a small scale and highly specialized. Astonishingly, only two companies in the world are dedicated to global distribution of their vaccines [6]. This seems to be in part because global distribution is costly and highly regulated, making it unprofitable for small companies. The largest challenges associated with vaccine production and distribution are in legal and regulatory issues. Legally, companies are unable to sell or distribute vaccines to a country until approval of the vaccine is obtained. Requirements for approval range from adequate manufacturing processes and facilities to allowing regular inspections of production practices [6, 7]. Each country or region has its own set of rules and requirements, making the approval process for globally-distributed vaccines arduous and costly. Once approval is obtained, vaccine production can be scaled up. The most common manufacturing method for many vaccines, including the flu vaccine, uses chicken eggs to grow vaccine viruses, which can then be purified from the egg white [8]. Clearly, this process is not without limitations, one of which is that millions of eggs must be harvested to create vaccines for large populations, creating a shortage of eggs and driving up the price. This is especially problematic in developing countries. Thus, cell-based production using synthetic biology and recombinant DNA vaccines are becoming increasingly widespread as a cheaper and more accessible method. To ensure safety, each batch of vaccines are carefully tested for sterility and protein concentration according to the WHO standards. It can then be packaged for use in humans. In most countries, clinical studies must be done in a small group of people before the vaccine can be made available for the public. For the flu vaccine, this has largely become routine, but is a major hurdle for manufacturers of novel vaccines. At the brink of a possible epidemic, the testing and regulatory process is often sped up, with WHO and governments shunting extra money into vaccine development. In the best case scenario, WHO estimates that a vaccine can be completed, tested, and distributed in five to six months [5]; however, some diseases are harder to crack than others, and the timeline may be longer for viruses like Zika. Even for influenza, the most well-characterized vaccine, the process is difficult. Each yearly flu shot consists of different strains and chemical components specific to that year. Almost immediately after a year’s flu season, the research restarts. Researchers begin selecting the most probable strains of a virus for the upcoming year and start preparing vaccine production by March. Release of the year’s vaccine may be as early as July, with distribution coming soon after. 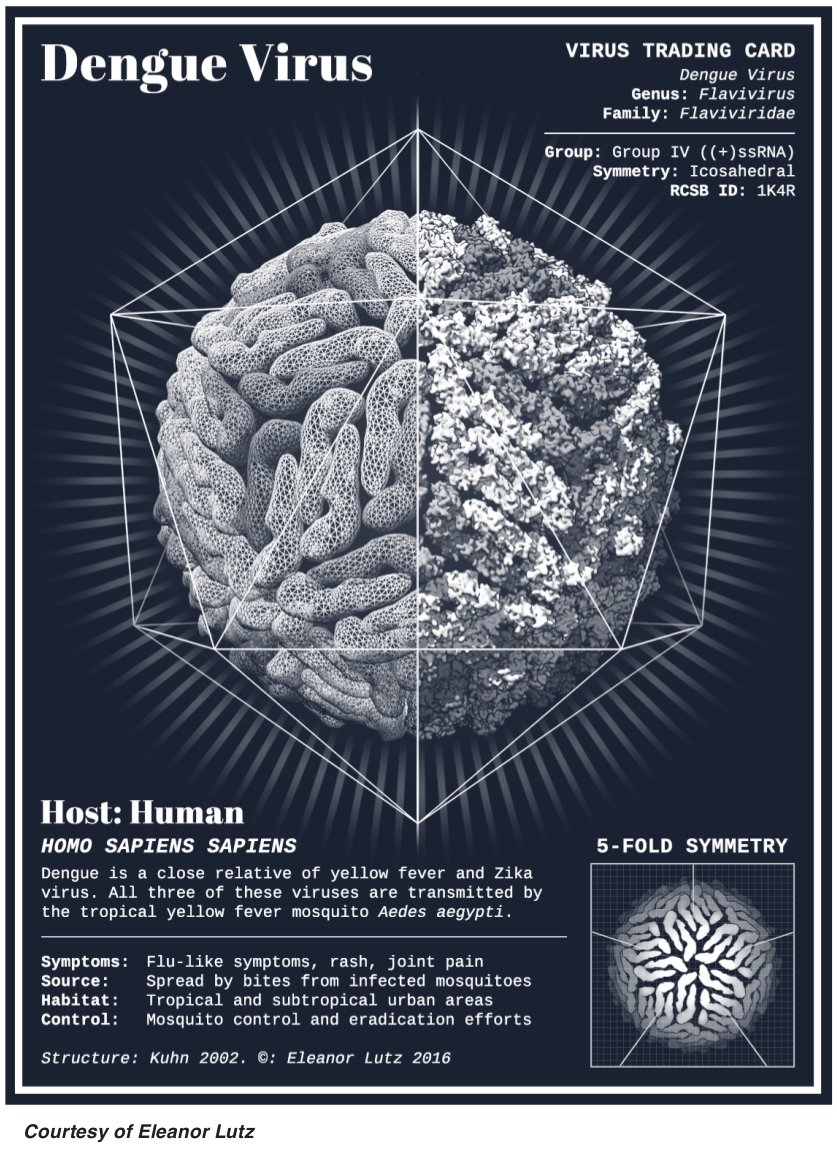 Race For a Zika Vaccine Zika virus is a flavivirus, similar to dengue fever, yellow fever, and West Nile virus [9]. First isolated in monkeys and mosquitoes in 1947 in Uganda’s Zika Forest, it has since appeared in multiple forms in other African nations, Southeast Asia, the Pacific Islands, and South America. It is most commonly transmitted to humans by mosquitoes, though a few cases of sexually-transmitted Zika virus have been documented in the most recent outbreak. Symptoms usually appear as a low-grade fever, rash, eye irritation, or joint pain, though only about 20% of patients experience noticeable symptoms. While Zika is generally not a serious risk to children and adults, it has been associated with miscarriage or severe birth defects in children whose mothers were infected during pregnancy [9]. According to one Brazilian study, of 42 pregnant women shown to be infected with Zika, 29% showed fetal abnormalities on ultrasound imaging. Beyond minimal studies of this kind, little is known about the spectrum of outcomes associated with the virus, and the biological chain of events leading to birth defects like microcephaly are not well understood. Additionally, there is some evidence that exposure to Zika virus can increase risk of Guillian-Barré syndrome, a severe autoimmune disorder in which the immune system attacks the nervous system, in some patients causing permanent nerve damage leading to perpetual weakness, numbness, and fatigue. As soon as the risks associated with the latest outbreak were identified, researchers began to work on a variety of preventative solutions, from developing vaccines to genetically modifying the carrier mosquitoes [10]. At the same time, governments have discouraged travel to affected areas and global health organizations have worked to educate the public, especially pregnant women, about the potential risks. Education campaigns have stressed the importance of birth control and protection from mosquito bites. Still, there is a significant need for a vaccine effective for pregnant women in high-risk regions. While effective vaccines exist for yellow fever and other viruses from the flavivirus group, no viable Zika vaccine has been produced at this time. As of May 2016, however, 18 different companies and research groups are working towards developing a Zika vaccine [9]. These groups are developing vaccines of varying types, including inactivated, recombinant, and DNA vaccines. One group is using two different approaches to develop two parallel vaccine candidates. India’s Bharat Biotech started working on a Zika vaccine in November of 2014 as an extension of their work on dengue fever and other flaviviruses, before the most recent outbreak began [11]. Their first candidate is an inactivated vaccine, which contains whole Zika virus particles that have been “killed” using chemicals, heat, or radiation so that they can no longer replicate or cause infection; however, because they contain most of the Zika DNA and proteins, they trigger a similar immune response to the natural virus [11]. One major advantage of an inactivated vaccine is that it doesn’t require refrigeration and can easily be freeze-dried for transport, making it ideal for use in developing countries [3]. Inactivated viruses are known for their safety and genetic stability compared with live viruses and the efficient immune response they produce. However, one disadvantage is that they require booster shots later in life to maintain a patient’s immunity. The second vaccine being developed by Bharat Biotech is a recombinant vaccine, which is produced by inserting the Zika DNA into an innocuous viral vector, a virus genome that has been “attenuated” and thus does not cause disease in humans [11, 12]. Essentially, the recombinant Zika vaccine does not contain the full Zika virus, but contains certain regions of DNA targets from the virus that can activate the specific immune system. Recombinant vaccines avoid several obstacles to production and potential safety risks. For example, they generally have less risk of a side effects and reactions than live or inactivated viruses. Recombinant vector vaccines closely resemble a natural infection and can stimulate a similar immune response. Additionally, recombinant viruses can reproduce in the body and there is some thought that booster vaccines later in life will be unnecessary, as the patient will continually have both the virus and compatible immune components in their bodies long past the initial vaccine. Both of these vaccines are still undergoing animal and human trials, which are long and painstaking in order to ensure patient safety. According to Dr. Krishna Ella, CEO of Bharat Biotech, it may be years before either vaccine can hit the market [11]. The exact timeline depends significantly on how much support they can garner from the World Health Organization and other groups, and the approval process from national health administrations (such as the FDA in the United States). Pennsylvania-based company Inovio Pharmaceuticals is another company working towards a Zika vaccine [13]. Theirs is a DNA vaccine, in which DNA is injected into the body and taken up by some of the patient’s cells, which then express proteins that the DNA codes for on their surfaces and induce an immune reaction against them [14]. Thus, the body’s own cells essentially become vaccine manufacturing plants, producing both the antigens and the resulting immune response. In mice, this vaccine has proved promising, producing a robust antibody and T cell response. The company plans to begin testing the vaccine in humans by the end of 2016, but it will likely be a few years before it makes its way to market. Summary Although the public may not often appreciate the rigorous process vaccines undergo prior to distribution, vaccine research has a huge impact on society. In a world with constant evolution of new and potentially deadly virus strains, bioengineers and epidemiologists are on the front lines, working quickly to identify pathogens and develop new vaccines while ensuring the safety and efficacy of their products.
0 Comments
Leave a Reply. |
Author
Articles written by members of the group on topics they find interesting, exciting, revolutionary. Archives
February 2018
Categories
All
|

 RSS Feed
RSS Feed
